Phimosis is a condition where the foreskin is too tight to be retracted over the head of the penis. In adults, it can cause pain during sex, difficulty urinating and recurring infections. Treatment options in the UK include topical steroid cream, foreskin stretching exercises, preputioplasty and circumcision. Steroid cream combined with stretching is usually the first step, with surgery recommended when other treatments have not worked or scarring is present.

Phimosis is when the foreskin cannot be fully pulled back over the head of the penis. In babies and young boys, this is completely normal. The foreskin separates gradually, and most boys have no tightness at all by their mid-teens.1
If you are an adult and your foreskin will not retract, or if it has started causing pain during sex or when urinating, that is worth getting checked. It usually is not serious. But it is unlikely to resolve on its own.
This guide explains what phimosis is, what causes it, how it is graded, and what treatment looks like in the UK, including both NHS and private options. It is for information only and does not replace a conversation with a clinician.
What is phimosis?
Phimosis, from the Greek for ‘muzzled’, is the medical term for a tight foreskin that cannot be retracted over the glans (head of the penis). The NHS defines it as a foreskin that is difficult or impossible to pull back.2
There are two distinct types. Understanding which one you have matters, because the treatment approach is completely different.
- Physiological phimosis: normal in babies and boys up to around 16. The foreskin detaches gradually as the child grows. No treatment is needed unless it is causing symptoms.
- Pathological phimosis: develops in adolescence or adulthood, usually because of scarring, infection or a skin condition. This is the type that needs treatment.
A tight foreskin in a seven-year-old is almost never a cause for concern. A tight foreskin that develops or persists and worsens into adulthood usually is.
Phimosis symptoms
Not every tight foreskin causes problems. Some men go years without noticing any difficulty, and the condition only becomes apparent during sex or a routine examination.
When symptoms do appear, the most common are:
- Inability to retract the foreskin over the glans
- Pain or discomfort during erections or sex
- Soreness, redness or swelling of the foreskin or glans
- A weak or disrupted urine stream, or foreskin ballooning when urinating
- Recurrent urinary tract infections (UTIs)
- Discharge or odour from beneath the foreskin
- White scarring or thickening of the foreskin skin, which may indicate lichen sclerosus
If you are getting recurrent infections, having pain during sex, or finding urination difficult, see your GP or a specialist. Symptoms that come on suddenly, particularly swelling or difficulty passing urine, should be reviewed promptly rather than monitored at home.
What causes phimosis?
The cause depends on which type of phimosis you have.
Physiological phimosis
In babies, the foreskin is naturally attached to the glans and non-retractile. It separates gradually. Most boys have full retraction by 14 or 15, and for some it can take until 17 or 18. This is normal and does not need treatment unless it is causing real problems.3
One common mistake worth flagging: attempting to retract a child’s foreskin before it is ready causes small tears that heal as scar tissue. That scar tissue can create pathological phimosis later. Leave it alone unless a clinician advises otherwise.
Pathological phimosis
When phimosis develops or worsens in adulthood, there is usually an identifiable reason. The most common causes are:
- Lichen sclerosus (BXO): a chronic inflammatory skin condition that causes hard, white scarring of the foreskin. It is one of the most frequent causes of acquired phimosis in adult men, and it does not respond well to steroid cream or stretching alone.4
- Recurrent balanitis: repeated inflammation of the glans, usually from infection, leads to scarring over time.
- Forcible retraction or trauma: tearing the foreskin causes scar tissue to form, which tightens it further.
- Skin conditions: psoriasis, eczema and contact dermatitis can all affect foreskin flexibility.
- Poorly controlled diabetes: high blood sugar raises the risk of recurrent infections that cause scarring.
Your GP or a specialist can assess whether there is an underlying cause and arrange any relevant tests.
Phimosis stages and grades
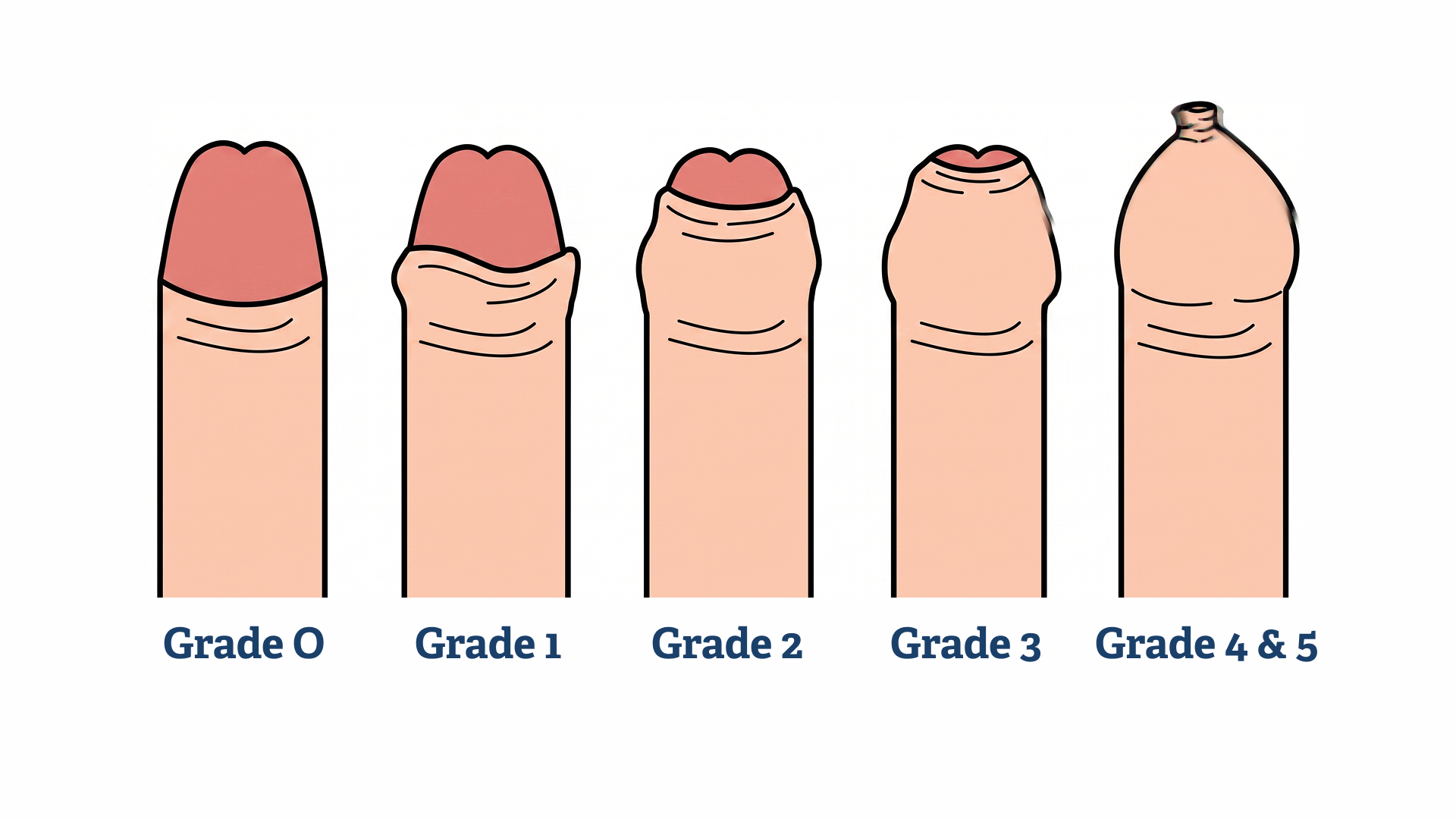
Phimosis is most commonly graded using the Kikiros classification, also called the Phimosis Index, which runs from Grade 1 to Grade 5.5 Your consultant will assess your foreskin at the first appointment and assign a grade. This guides the treatment recommendation.
| Grade | What the foreskin does | What it usually means |
|---|---|---|
| Grade 1 | Full retraction possible; mild tightness when retracted | Near-normal. Treatment rarely needed |
| Grade 2 | Partial retraction; glans partially visible | Mild phimosis. Steroid cream may be sufficient |
| Grade 3 | Retraction only as far as the urethral meatus | Moderate. Treatment likely required |
| Grade 4 | Partial retraction; glans not visible at all | Significant. Surgical treatment often recommended |
| Grade 5 | No retraction at all | Severe. Surgery almost always required |
Source: Kikiros CS, et al. The response of phimosis to local steroid application. Paediatric Surgery International. 1993.
- Concerned about phimosis?
Book a phimosis consultation in Birmingham
Our GMC-registered doctors will assess your foreskin, discuss your options and, where appropriate, carry out treatment at the same appointment. All procedures are performed under local anaesthetic with same-day discharge.
Phimosis treatment options in the UK
If your phimosis is mild and there is no scarring, steroid cream is usually the first step. If you have lichen sclerosus, cream almost certainly will not be enough and surgery is the more likely path. Your consultant will advise based on what they see at the appointment.
Steroid cream for phimosis
A short course of topical corticosteroid cream, usually betamethasone 0.05% applied twice daily for four to eight weeks, is the standard first-line treatment for mild to moderate phimosis where scarring is not the main issue.
A systematic review in the Journal of Urology found success rates of 67 to 95 per cent for topical steroid treatment in both children and adults with non-scarring phimosis6, roughly seven or eight in ten patients seeing meaningful improvement. It is significantly less effective where lichen sclerosus is the underlying cause.
Steroid cream is available on NHS prescription from your GP, or through a private clinic. Your clinician will advise whether it is appropriate before prescribing.
Stretching exercises
Gentle, regular stretching of the foreskin is usually recommended alongside steroid cream. It needs to be done consistently and never to the point of pain. Forcing it causes the small tears that lead to more scarring, which is the opposite of what you want.
When done correctly over several weeks, cream combined with stretching can avoid surgery in a significant proportion of cases.
Preputioplasty
Preputioplasty is a surgical option for men who want to preserve their foreskin. A small incision is made in the tight band to widen the opening, allowing normal retraction without removing the foreskin.
It is performed under local anaesthetic, takes under 30 minutes, and most men are back to light activity within a day or two. It is suitable when the underlying tissue is healthy. It is not recommended where lichen sclerosus has caused significant scarring, because scar tissue tends to re-tighten after surgery.
Risks include: bruising, swelling, infection and, in a small number of cases, re-tightening of the foreskin. Your clinician will discuss these before the procedure.
At Gentle Procedures UK, preputioplasty is offered as a day-case procedure at our Birmingham clinic.
Circumcision for phimosis
Circumcision is the definitive treatment for phimosis and is typically recommended when conservative measures have failed, when lichen sclerosus is the underlying cause, or when the phimosis is Grade 4 or 5.7
The NHS provides circumcision on medical grounds where clinically indicated. Your GP can make a referral if it is appropriate. Private circumcision means a fixed appointment date, a consultation beforehand and same-day discharge, without waiting-list uncertainty.
At Gentle Procedures UK, adult circumcision is performed using the Pollock Technique, a minimally invasive approach under local anaesthetic. Most patients go home the same day and return to light activity within one to two days.
Paraphimosis: a separate and more serious condition
Paraphimosis is a medical emergency.
If you or someone else has a foreskin stuck in the retracted position, causing swelling and pain, call 999 or go straight to A&E. Do not wait. Delayed treatment can restrict blood supply to the penis.1
Paraphimosis is not the same as phimosis. Phimosis means the foreskin cannot be pulled back. Paraphimosis is the opposite: the foreskin has been retracted and is now stuck behind the glans, causing it to swell rapidly.
When to see a doctor about phimosis
See your GP or a specialist if you or your child experience any of the following:
- Pain or difficulty urinating
- Swelling, redness or discharge from beneath the foreskin
- Pain during sex that is affecting quality of life or relationships
- A foreskin that has not retracted by the mid-teens and is causing concern
- White scarring or thickening of the foreskin skin
- Recurrent infections or episodes of balanitis
The earlier phimosis is assessed, the more options are available. Steroid cream works best before significant scarring has developed.2 Once lichen sclerosus is established, surgery is usually the only effective path, which is why early review matters.
Frequently asked questions about phimosis
Phimosis is the medical term for a tight foreskin that cannot be fully retracted over the head of the penis. The word is Greek for ‘muzzled’. It can be physiological, meaning normal in young children, or pathological, meaning it has developed due to scarring or a skin condition in later life.
Yes, in babies and young children. The foreskin is naturally tight at birth and loosens with age. Most boys’ foreskins retract fully by their mid-teens.1 It is only considered a clinical problem if it is causing symptoms or if it persists into adulthood without any improvement.
In children, physiological phimosis usually resolves naturally without treatment. In adults, pathological phimosis is unlikely to resolve on its own. Treatment with steroid cream, stretching or surgery is typically needed.
Yes. The NHS can prescribe topical steroid cream and, where there is a clinical need, refer patients for circumcision or preputioplasty.1 NHS waiting times for surgical treatment can be several months. Many men choose private treatment for a fixed appointment date and more flexible access.
Phimosis is diagnosed through a physical examination. Your GP or a specialist will assess how far the foreskin retracts and check for signs of scarring, infection or an underlying condition. No scans or blood tests are usually needed for a straightforward diagnosis, though further investigations may follow if lichen sclerosus is suspected.
References
- NHS. Tight foreskin (phimosis). Available at: https://www.nhs.uk/conditions/phimosis/ [Last reviewed: March 2026]
- Bunker CB. Male genital lichen sclerosus: a clinician’s guide. British Journal of Dermatology. 2021;185(4):691-700. Available at: https://doi.org/10.1111/bjd.20115
- Kikiros CS, Beasley SW, Woodward AA. The response of phimosis to local steroid application. Paediatric Surgery International. 1993;8(4):329-332. Available at: https://pubmed.ncbi.nlm.nih.gov/8108034/
- Ashfield JE, et al. Treatment of phimosis with topical steroids in 194 children. Journal of Urology. 2003;169(3):1106-1108. Available at: https://doi.org/10.1097/01.ju.0000045771.87226.49



